
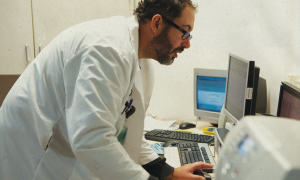
The San Diego Nuclear Medicine team discovered that the premise of their first performance improvement project—high repeats of heart scans—was not the problem they initially suspected. Above, assistant technologist and labor co-lead Jessica Larson (left) and technologist Christine Cook (right) assist patient Robert Evans. Larson and Cook are members of OPEIU Local 30.
Why teams that try and fail are better than teams that always succeed
"Anyone who has never made a mistake has never tried anything new."
—Albert Einstein
This is the story of a team that never failed a test of change. No matter what the team members did, rapid improvement cycle after rapid improvement cycle, every small test tried was a better jewel than the one before. They received an A for their PDSAs.
They were fearless—in their imaginations. The only problem with the team’s brilliant tests of change was that they never got tested, never got to the stage where stumbling or failed ideas might have real consequences. There was no learning, no innovation, no growth—just intriguing ideas that remained bottled.
In health care, it’s still frowned upon to talk about failures or things that don’t work out perfectly for fear the information will be used against the people involved. But even in a high-stakes industry where the consequence of some decisions means life or death, there is plenty of room for improving performance by learning from small failures.
Using small failures as learning opportunities is the cornerstone of creating a learning organization. Small failures are at the heart of the Rapid Improvement Model and its plan, do, study, act cycles.
“Despite the increased rate of failure that accompanies deliberate experimentation, organizations that experiment effectively…are likely to be more innovative, productive and successful,” writes Amy Edmondson, a professor at Harvard Business School, in a December 2004 article in the Quality and Safety in Healthcare Journal.
This in fact is a story of false starts: the story of unit-based teams and employees throughout Kaiser Permanente who already are learning, developing and innovating from missteps or downright unsuccessful small tests of change.
From projects that changed direction after data contradicted the original premise, to tests of change that were tweaked or abandoned all together, workers describe how they tried a small improvement that didn't turn out as expected and still gained from the experience. And even, eventually, found success.
Learning to fail
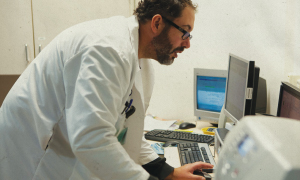 At San Diego Medical Center’s Nuclear Medicine department, the unit-based team decided its first test of change project would look at reducing the number of redundant heart scans, which technologists were certain were wasting time and resources.
At San Diego Medical Center’s Nuclear Medicine department, the unit-based team decided its first test of change project would look at reducing the number of redundant heart scans, which technologists were certain were wasting time and resources.
In November 2009, team members began to track the number of repeat scans to establish a baseline. They figured repeats would be at least 25 percent of the heart scans. After a month of logging the scans, however, they discovered something quite different.
“The number of repeat heart scans was actually between 7 to 10 percent,” says the UBT’s labor co-lead, Jessica Larson, a tech assistant and OPEIU Local 30 member.
The team’s hypothesis was amiss. It switched gears.
Since several of the staff recommendations for test of change projects related to heart scans, the team focused next on the variation in the instructions patients were given. If team members gave identical instructions, they might be able to all but eliminate repeat heart scans.
“The test of change at that point was to make sure everyone was following the protocol,” says Randy Andres, a nuclear medicine technologist and OPEIU Local 30 member.
The team created laminated handouts with one set of clear instructions that technologists and receptionists were to hand out to every patient before a scan.
“We did that for a few weeks, and found it was a lot more complicated than we anticipated,” Larson says. “You had inpatients, outpatients, observation-unit patients….Forms were getting misplaced because patients would leave them in the waiting rooms or in their purse. Or people weren’t even giving them out.”
During the same time, a supply shortage meant the department had to switch the type of injectable radioactive isotope it was using. The change meant a whole new set of protocols. Compounding it all, the department’s longtime manager retired.
It was time to shelve the test of change.
But was it a waste of time? Not at all, say Larson and Andres. Both say it provided valuable information about the department’s work flow—as well as practical knowledge of how to conduct tests of change.
“This was a very good teaching experience for us,” Andres says. “We didn’t even know about tests of change before this. It’s not simply a matter of just changing something. You have to go through this process.”
Too much of a good thing
Further north at Redwood City Medical Center, the Gastroenterology department discovered you can have too much of a good thing.
Contracting with an Oregon company that specializes in mass outreach calls, the department began using automatic robocalls to reach patients ages 50 to 75 who were due or overdue for colorectal screenings.
“We had to think outside the box,” says Julie Dalcin, director of medicine. “This was a way to reach a lot of people.”
The first round of robocalls went out in November 2009, with some 10,000 calls made. They reached 97 percent of the members who were due for the tests—but there was a problem. The calls were made within a span of three hours, and the response overwhelmed the department and the facility. The voicemail box the team had set up in advance barely helped; it could take only 50 messages.
“We got bombarded by calls from patients calling back with questions or requests. Our operator was inundated,” says manager Isabel Uibel. “Physicians in other departments were also bombarded with calls. People…were like, ‘What’s going on?’”
Michele Coons, a medical assistant and SEIU UHW member, was devoted to returning the calls and to mailing “FIT kits,” the at-home stool tests that help detect early signs of colorectal cancer, to those who had requested them.
“Many people had a lot of questions,” Coons says. “‘Why did I get this call?’ ‘What does a FIT kit test mean?’”
It took a week to figure out a system for getting back to all the patients, she says.
“I think at the end of day you have to be willing to try,” Uibel says. “And forgive yourself for the time you put into something that didn’t work. And don’t lose motivation. But also know when…you’ve got to say, ‘We’re not going down the right path at all.’”
In some workplaces, what had happened would be labeled a disaster. But not in Redwood City. The essential idea was sound. For the second round of calls, the team addressed the overwhelming response by having the calls made over a two-week period.
“We didn’t think we needed to throw the baby out with the bathwater,” Uibel says. “We just had to keep tweaking to make the system work for us.”
Too good to be true
When it came to how quickly patient messages are responded to, the Internal Medicine at the East Denver Medical Office in Colorado was pretty close to bottom—only 8 percent of patient advice calls were answered within an hour. The team members were open to trying anything, and after several small tests of change, they hit on something so ridiculously simple that some people resisted it.
Nurses tape neon orange cards with the patient message to the door of the exam room where the doctor is working. The doctor sees the message on the way out of the room and goes back to his or her office to respond.
Within the first three months of the test, the department saw message turnaround times soar to 30 percent answered within the hour.
“You had some tangible symbol that you were trying to make these numbers move. It was a great motivator,” says Christopher Hicks, MD, the team’s physician co-lead. “It was different. It wasn’t something that was happening electronically.”
Then they hit a wall.
“We were sitting around threshold or target and then would drop back down,” explains Olivia Wright, supervisor and management co-lead. “We were just hovering around 20 to 30 percent.”
The team brainstormed about why it couldn’t move the number above 30 percent.
Someone suggested one reason could be that the call center opened at 7 a.m. and most of the staff didn’t start until 8 a.m. They were starting the day already behind the curve with waiting messages. Two nurses changed their schedule and started coming in at 7:30 a.m. That seemed to help: 52 percent of patient messages got a reply within an hour.
“You’ve got to give something a shot,” Wright says. “The first thing you come out of the gate with isn’t necessarily going to be the end-all be-all, but you’ve got to start somewhere.”
One of the most surprising lessons for the entire department was the fact that small changes could have such a large impact.
“There was a sense of disbelief,” Wright recalls. “We had to reassure the team that the volume of work hadn’t gone down or that it wasn’t because of the time of year. We’ve sustained these results since May, and it finally started to sink in that small, subtle changes really are the reason for these results.”
Failure is part of experimentation
 Experts who study organizations like health care and the airline industry corroborate the importance the process of experimentation plays in organizational learning.
Experts who study organizations like health care and the airline industry corroborate the importance the process of experimentation plays in organizational learning.
“Under conditions where there’s a lot of uncertainty and constantly moving parts and work is customized or unique, the only way to make it work is to allow the right level of leeway for teams…to experiment thoughtfully,” Edmondson says. In the long run, lasting success comes from a willingness to try new things; but, if you try new things, you're going to fail sometimes.
This isn’t license for projects based on haphazard hypotheses, but it underscores the fact that performance improvement methods such as the Rapid Improvement Model are made for small failures. Because the process allows for quick experimentation, with results evaluated within 30 to 60 days, there is little to lose.
Barbara Grimm, senior vice president of the Labor Management Partnership, would have people ask themselves a few questions that can help them weigh the possibility of failure.
“Have you reasoned through the consequences? That is key,” Grimm says. “Do you have the patient’s interest absolutely there? Do you have a plan if it doesn’t go well?”
Edmondson argues there are two key reasons health care organizations still resist learning from small failures: The culture often discourages questions, challenges, or admissions of error, and a demanding workload and pace force staff to rely on quick fixes when something doesn’t work, instead of systematic problem solving.
That is changing at Kaiser Permanente with the commitment to providing frontline staff with training and support to conduct root cause analysis and problem solving with RIM, RIM+ and other performance improvement tools. And unit-based teams give staff members the place and time to do this work.
John August, executive director of the Coalition of Kaiser Permanente Unions, believes the
true purpose of the Labor Management Partnership is to recognize the mission of KP and the mission of the unions are at profound risk due to the economic, competitive and public policy environment in which we operate.
“We must continually remind everyone in the organization that the why of what we do in partnership is driven by this fundamental recognition and agreement,” August says. “If we don’t make the effort to discuss the reasons why we’re doing this, people will get the impression that people are just being asked to do something. And being asked to do something doesn’t create an atmosphere of safety.”
Edmondson says the sense of safety will further develop when we learn to accept and work with our limitations.
“People need a sense of psychological safety, and frankly a sense of humor about our humanness,” Edmondson says. “Somewhere along the line we get socialized and begin to buy into the absurd notion that we should be perfect.”
Back at the lab
In San Diego, Larson thinks even if the tests of change didn’t work exactly as planned, it gave the team something even more important—the beginning of a different work culture.
“Being able to work on small tests of change enabled us to get past what’s always been,” Larson says. “There are people who have been here longer than I’ve been alive and so are accustomed to the way it was always done. But trying something new can save us time, and save the company money, and can be better for the patient. So I found it nice to look at it like, ‘Let’s try just this little thing and it might just make it better.’”
Larson is certain the eventual reward will outweigh any frustrations in wrong hypotheses or failed tests.
“Either you find you can fix something or you can’t, and you just move on,” Larson says. “Just keep trying. Because ultimately, it’s going to be a success in the end.”